
Prof. Brian Norton,
DLA member
20 May 2020
Introduction
The COVID-19 pandemic continues to ravage societies with deep, often tragic, psychological, social and economic consequences. Across the world, extensive precautionary social distancing measures have repurposed how many buildings are, or will be, used as well as how many cities now operate. These changes have been rapid, diverse, sometimes extreme but often trivial, surprising and unexpected. Immediate vicissitudes range from working and educating from home, the reduced occupancy of supermarkets and public buildings, less use of public transport but increases in delivery traffic. This has led to changes in patterns of energy and transport use that have, in many places, improved outdoor air quality and reduced greenhouse gas emissions. As economic activity recommences in the absence of vaccines or proven treatments to stem the spread of COVID-19, further, and probably profound, permanent changes to our built environments will become necessary.
That pandemics necessitate adaptation is not new. One example of large-scale citywide infrastructural innovation is how the 1848–49 and 1853 cholera epidemics in which 25,000 people died, led to London’s first main sewer network in the 1860s. This not only eliminated cholera in the water system, whilst also decreased subsequent typhus and typhoid epidemics. An example of driving change at the buildings scale is the introduction in Hong Kong in 1903 of building regulations to improve sanitary standards and reduced overcrowded housing by placing greater emphasis on space, fresh air and daylight to avoid the rapid spread of diseases as had occurred when 20,000 people died in a Bubonic Plague outbreak in 1894.
Light, air, buildings and space
Light in medical treatment has its scientific origins in phototherapy lamps, a Nobel prize winning, treatment for tuberculosis (Finsen, 1893). Sunlight with the appropriate spectrum and intensity may provide viral sterilization. Hope-Simpson (1981) noted that changes in average solar radiation intensity correlated with the seasonality of epidemic influenza. This is due to ultraviolet radiation, specifically UV-B in the wavelength range 280nm to 315 nm promoting vitamin D production in the skin in summer with conversely a vitamin D deficiency ensuing in winter (Cannel et al, 2006). In respiratory tract linings, Vitamin D stimulates cells that may partially shield lungs from infection. With a strong caution that correlation does not necessarily mean causality, one recent small-scale non-randomised study in Jakarta, Indonesia may indicate that solar radiation intensity correlated significantly to Covid-19 patients’ recovery (Asyary and Veruswati, 2020) perhaps by enhancing vitamin D production that counteracted suppression of the immune system. There remains a need for large-scale randomized trials to determine the validity, and then effectiveness, of this hypothesis.
Exposure to UV-B can inactivate viruses, including the SARS-CoV-2 virus, but requires over an hour’s exposure to do so, even under the highest solar radiation intensities obtainable under very clear sky conditions (Hauser, 2020) with considerably longer exposures required at lower solar radiation intensities. However, this is not appropriate for virus inactivation on the skin, as UV-B is harmful. Artificial ultraviolet light sources predominantly emit in the UV-C range particularly dangerous to skin and eyes. UV-C, the most effective virus-inactivating type of UV radiation, does not form part of the solar spectrum; being at wavelengths from 100 nm to 280 nm, UV-C stops virus replication by damaging RNA sequences. It is also notable that some UV light is not particularly dangerous or beneficial; UV-A, in the wavelength range from 315 nm to 400 nm, neither generates vitamin D nor is significantly harmful to either people or to viruses. More speculatively, in animal experiments, red and near infrared light reduces respiratory disorders similar to those associated with coronavirus infection. In patients, red light may alleviate chronic obstructive lung disease and bronchial asthma (Enwemeka, et al, 2020). Again, this requires much further research. If such effects are found to be significant, they may have implications for the best wavelength selectivity for building glazings.
High urban densities can mean shorter, walkable or cyclable, travel distances to work thus avoiding both close contact in public transport and environmentally unsustainable use of private cars. However, the high density of high-rise buildings in many cities present major challenges in avoiding close social contact and cross contamination. Pathogens can be transmitted by plumbing (Gormley et al, 20017) and ventilation (Dietz et al, 2020) systems. In building ventilation systems, transmission of air-borne viruses associated with much larger water and protein particles may be reduced by finely meshed filters (Dietz et al, 2020). However smaller particles penetrate even fine meshes, recirculation of air within a building is inadvisable. Continuously introducing fresh air into buildings via windows and/or HVAC systems prevents recirculation of air-borne viruses, but increases heating costs. Building integrated use of solar energy to pre-heat ventilations air in winter can alleviate much of this increase in costs while reducing the carbon footprint. Increased cooling ventilation will also be required in the much hotter summers arising from climate change. Ventilation air flow rate increases of 0.4 ms-1 per 0C ambient temperature elevation to prevent increased deaths from heat-stress.
In many parts of the world, rapid urbanisation has produced open spaces that are limited both in extent and quality. City parks and other dedicated open spaces give access to sunlight and fresh air. Health maintenance may become their key function; rather than perhaps being an inadvertent consequence of areas often provided primarily for children’s exercise, as part of urban planning requirements or simply by historical accident. In order for designers to accentuate those benefits, further formal research is necessary to quantify the health attributes of open spaces.
Conclusion
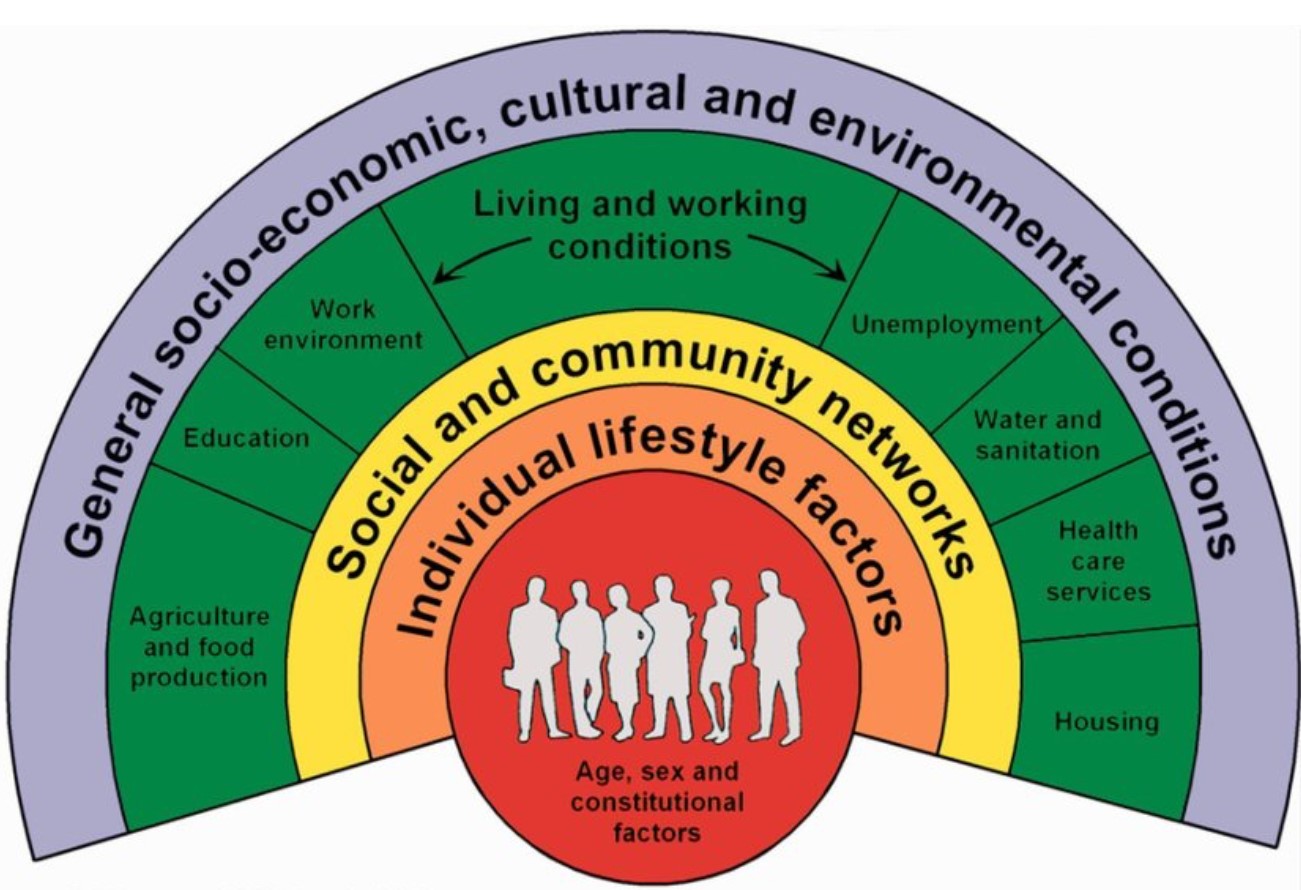
Pandemics, similar to COVID-19, may occur more frequently, may be more extreme and may endure longer. It is equally possible that climate change may lead to new unknown diseases. It would thus be precautionary wisdom to incorporate the lessons learned in COVID-19 to the future design of buildings and spaces. There are many apparent contradictions requiring resolution. Holistic multidisciplinary perspectives are therefore critical to successfully examining these challenges. These complex interactions, as embraced in the World Health Organisation’s definition of a healthy city (WHO, 1998), are captured in the diagram in Figure 1.
Directly and indirectly, pandemics have a long history of being a driver of innovation from urban-scale infrastructures to the minutiae of regulatory standards applied to the planning, design, and construction of individual buildings. Our buildings and cities need to be designed to provide physically and psychologically healthy and disease-averting indoor and outdoor spaces. Low-risk built environments will be critically valuable to the elderly, who have been particularly vulnerable to, and most isolated by, COVID-19.
References
A. Asyary and M. Veruswati (2020) Sunlight exposure increased Covid-19 recovery rates: A study in the central pandemic area of Indonesia, Science of The Total Environment, 729, 139016.
J.J. Cannell, R. Vieth, J.C. Umhau, M.F. Holick, W.B. Grant, S. Madronich, C.F. Garland, E. Giovannucci, (2006) Epidemic influenza and vitamin D, Epidemiology and Infection, 134, 1129-1140.
G. Dahlgren and M. Whitehead (1991). Policies and Strategies to Promote Social Equity in Health. Stockholm: Institute for the Futures Studies.
L. Dietz, P. F. Horve, D. A. Coil, M. Fretz, J. A. Eisen, K. Van Den Wymelenberg,(2020) 2019 Novel Coronavirus (COVID-19) Pandemic: Built Environment Considerations To Reduce Transmission, mSystems 5.
C. S. Enwemeka, V. V. Bumah and D. S. Masson-Meyers (2020) Light as a potential treatment for pandemic coronavirus infections: A perspective. Journal of Photochemistry and Photobiology B: Biology. In press.
N. R. Finsen, (1893) Om Lysets Indvirkninger paa Huden (On the effects of light on the skin), Hospitalstidende, 36, 721–728.
M. Gormley, T. J, Aspray, D. A. Kelly and C. Rodriguez-Gil (2017). Pathogen cross-transmission via building sanitary plumbing systems in a full-scale pilot test-rig, PLoS ONE 12(2).
R. E. Hope-Simpson, (1981). The role of season in the epidemiology of influenza. J Hygene (Lond). 86, 35–47.
K.W. Houser, (2020) Ten Facts about UV Radiation and COVID-19, LEUKOS The Journal of the Illuminating Engineering Society, 16, 177-178.
WHO (1998). Health Promotion Glossary.
https://www.who.int/healthpromotion/healthy-cities/en/
Very useful information.
Would expect noting else from Yourself Professor. Kind regards.